

"there is no evidence that the use of masks in public will protect an individual from infection"
A quote from University of Guelph's COVID-19 Pandemic Plan

It has been two years, six months, and twenty-six days (938 total days) since the administration of my employer, the University of Guelph, banned me from accessing my office and laboratory. I spoke truths about COVID-19 when much of the world was not ready to hear them. As the University of Guelph still expects me to work, I would like to have access to my work spaces. Segregation makes me feel less than human.
- B. Bridle -
As a result of widespread confusion about how to respond to the swine influenza pandemic that was declared in 2009, all publicly funded institutions in Canada were required to establish pandemic plans. This was done outside of the context of a pandemic while calm minds prevailed to ensure that the overall weight of the scientific evidence could objectively be incorporated into plans. What many Canadians still don’t seem to realize is that these ‘best laid plans’ were promptly discarded when the COVID-19 pandemic was declared. This occurred within all publicly funded institutions from the federal government down.
As an example of what these plans looked like, let me show you the plan that was supposed to be implemented at my university. What follows are quotes taken from the plan that is still on public file today at the University of Guelph, along with my observations.
“In 2020, the concern is the novel corona virus Covid-19.”
and
“send students home if they become infected with Covid-19“
and
“symptoms of Covid-19 infection“
This tells me that a competent virologist was not consulted when writing the plan. The novel virus was not “COVID-19”. COVID-19 is a disease that some people get following infection with the causative virus. One does not become infected with COVID-19, one gets infected with severe acute respiratory syndrome-coronavirus-2. An evident lack of oversight of the writing of this document by subject matter experts is concerning.
“This virus can infect a person and result in no apparent clinical disease, OR mild respiratory disease as would occur with the common cold, OR in others serious clinical illness leading to death. Current evidence is that those most seriously affected are older or have pre-existing health conditions.”
Excellent. I agree. The higher risk demographics were well-known and it was known that many people would not get sick or only mildly so. This was an excellent rationale for focusing measures on those at greatest risk, NOT a ‘one-size-fits-all’ approach. Unfortunately, history tells us that this logic was thrown out.
“Social Distancing
it is recommended that individuals be 2 meters apart”
and
“Infection Control Measures
maintain one metre distancing”
(bolding added for emphasis)
Contradictions like this cause one to lose confidence that distancing was based on a solid scientific rationale. A lack of consistency like this is more typical of an arbitrary selection of numbers.
“People can spread the virus prior to experiencing clinical signs of disease, and the mode of transmission is from droplets (sneezes and coughs).”
The contradiction here is obvious. How can someone that is NOT “experiencing clinical signs of disease” transmit a bolus dose of the virus that is sufficient to overwhelm the innate immunological defences of another person if “the mode of transmission is from… sneezes and coughs”, which are “clinical signs”. This is an implicit admission that sick people are the dominant transmitters of infectious diseases.
The concept of asymptomatic transmission as an important driver of spread of infections is false. I previously explained why this is.
A blatant contradiction like this gives the impression that this pandemic plan was not approved by a competent expert in infectious diseases.
“One possible approach would be setting aside residence blocks for students who are ill and unable to return home. However, this will require moving healthy students to other areas.”
I agree; sick people can spread diseases. Healthy people, which are those who are asymptomatic do not need to be isolated from other healthy/asymptomatic people. So, why was this logic not adhered to?
“4. Infection Control Supplies and Estimating Requirements
The use of masks and N95 respirators during a pandemic is determined based on a risk assessment of the level of care one would provide to a person exhibiting respiratory symptoms or the frequency of necessary and unavoidable face-to-face interactions between two individuals. According to the Canadian Pandemic Covid-19 Plan, there is no evidence that the use of masks in public will protect an individual from infection.”
[bolding added for emphasis]
Whoa!?! This completely contradicts the masking mandate that the university implemented! It has long been established now that this is a hotly debated topic among scientists, with broad agreement that studies looking at this are generally of very poor quality and, therefore, at high risk of bias. Nobody would possibly mandate something for healthy people unless there was unequivocal proof that the benefits substantially outweigh harms, would they?!?
“Collaborate with subject matter experts on pandemic planning to help with the development of accurate and timely messages, before and during a pandemic.”
I have already identified evidence that competent key experts were likely not consulted when writing the pandemic plan. And I can assure everyone that the senior immunologists on campus that closely followed the avalanche of scientific data were never consulted, despite immunologists being the pre-eminent experts on the sub-discipline of vaccinology.
“The members of the Campus Control Group (CCG)… must also consider additional issues unique to a pandemic including… Ensuring that actions taken to mitigate impact of the pandemic are not contrary to law”
and
“Legal counsel will be called on to provide advice on legal issues (e.g., restricting access or travel, isolation/quarantine, liability, compulsory vaccination for students, and prohibition of mass gatherings).“
(bolding added for emphasis)
First, note that any compulsory vaccination did not involve staff or faculty. Yet staff and faculty were mandated to take the COVID-19 shots, resulting in some losing their jobs and others suffering serious adverse events.
Me, along with two other senior immunologists bore witness in an online meeting to a vice-president of the University of Guelph stating in no uncertain terms that the university’s legal counsel had advised against implementing a vaccine mandate for anyone, including students. The university contravened this advice and implemented a mandate for the entire campus community, costing many students who did not want the COVID-19 shots a university education. Some of the students that felt coerced into taking the shots suffered severe adverse events.
I have witnessed individuals on my campus experience serious side-effects following receipt of COVID-19 shots under coercive pressure. As one example, let me share for the first time an anonymized case. Note that people on my campus cannot be identified due to extreme fear of repercussions. Here is the case as described in the person’s own words…
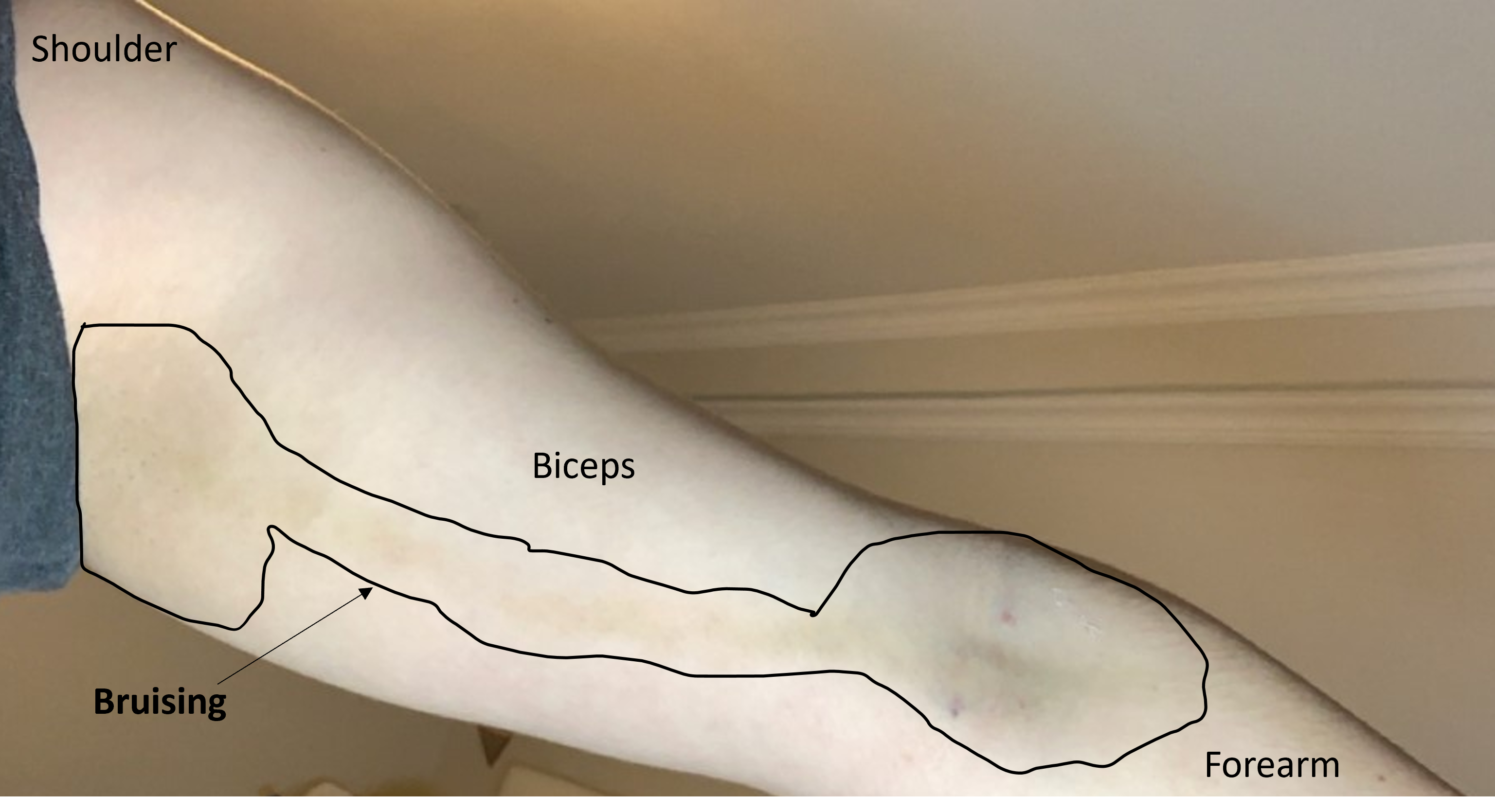
“I had my first dose of the Pfizer vaccine in my left arm on April 27th, and started experiencing side effects almost immediately (numbness, extreme vertigo, swollen lymph nodes, etc). By Friday April 30th, I had intense nerve pain down my right arm. By Monday May 3rd, the pain had become so intense, and I had a massive discolouration (see the attached picture below), that I went to the ER here in XXX. They did an ultrasound and of course, saw a deep vein thrombosis in my upper right arm, correlating with the discoloration. The discolouration was much darker in person, but due to bad lighting this is as good as the picture can get.
I have an MSc in Cell and Molecular biology, and my undergraduate degree was in biology and genetics; because of this, I have been EXTREMELY interested in how the mRNA vaccines could have caused clotting. Because even after the thrombosis clinic did a 2 hour long medical background check, they determined I have zero factors that increase my chances of clotting. I also do not even take any XXX, so there is literally nothing to blame this on. I think it goes without saying that it is too much of a coincidence for this to be anything but a direct reaction to the Pfizer shot.
Over the weekend a friend sent me a link to the podcast you were recently featured on, where you discussed an upcoming paper you and a team of collaborators are working on, which is how I was introduced to you. In the podcast you said that the mRNA vaccines, in rare cases, are causing some of the spike proteins to be released into the bloodstream, where they cause inflammation, and subsequently bloodclots in some cases. I strongly believe now this is exactly what happened to me. However, as far as I know, was never tested for the presence of these spike proteins, because the medical professionals at the thrombosis clinic did not believe it was Pfizer related. They said that it couldn't be ruled out as a possible. [Note: this is precisely why this should have been submitted to Canada’s adverse event reporting system. Physicians were NOT to make their own determination of whether a medical incident was related to the shots. In this case, like many others that I know about, a report was not submitted. Examples like this are how we know that adverse events were under-reported. Physicians that failed to report are at least indirectly responsible for harms not being identified in a timely fashion.]
I should mention that I ended up going back into the hospital on April 28th for the second time, after I started having severe chest pains. I didn't have a VQ scan done until over a week later (after being on Eliquis for that length of time), where it came back normal. The thrombosis doctor said that it didn't rule out the possibility that a clot was ever there- but because I had been on a double dose of Eliquis for over a week at the time of the scan, a small clot may have already broken up by then. These chest pains have now almost gone away entirely, however if I overexert myself, they do seem to come back slightly. I have never experienced this before until after this blood clotting incident, so I'm sure this must be related somehow.”
Here is the bruising in the arm…
Hundreds of people both on and off campus shared similar stories with me because they knew that I was a legitimate expert who accepted the fact that the shots were likely not entirely ‘safe and effective’. How could I have a conscience and not speak up when I was witnessing this over and over?!? For some reason many of my colleagues were over-the-top upset that I spoke the truth about this. But with so much harm occurring and the victims being afraid to say anything publicly, I would do it again despite the suffering I have had to endure.
Silencing of victims through fear of repercussions is not something that I should be expected to tolerate.
Reference Material:
University of Guelph’s COVID-10 Pandemic Plan…
This plan was to be executed by what is known as the “Campus Control Group (CCG)”.
This is from the University of Guelph’s Emergency Management Plan that was in effect at the beginning of 2020:
THE CCG CONSISTS OF THE FOLLOWING MEMBERS
1. Chair -VP of Finance, Administration and Risk Management or alternate,
2. Scribe for the Chair
3. VP External or alternate,
4. Provost and VP of Academic or alternate,
5. Associate VP of Student Affairs or alternate,
6. Associate A VP of Physical Resources or alternate,
7. Director of CCP, Emergency Management and Fire Safety or alternate,
8. Manager of Emergency Planning and Administration or Alternate,
9. Associate VP of Human Resources or alternate,
10. Associate VP of Financial Services or alternate,
11. Assistant VP of Communications and Public Affairs or alternate,
12. Director of Environmental Health and Wellness or alternate
Incident command system:


It's only been in the last few days I suddenly grasped just what sort of ethical / moral abomination the very notion of "Vaccine Mandates" truly are. Stop and think for 20 consecutive seconds about the ideas of:
1. Mandated lobotomies for all persons diagnosed with "depression."
2. Mandated administration of Thalidomide for all pregant women.
"Ridiculous", "outrageous", you say? Historically in both cases we came pretty close!
Thus so is the coercive administration of an untested, unapproved, unlicenced, irreparable injection intended to reprogram the human body's biology at the chromosomal level – after a deliberate months long terror campaign over an illness which – if it ever existed and I very much have my doubts – had a demonstrated mortality rate of 0.007%: You're in more danger of death driving to work every day! Under the original terms of The Nuremberg Code everyone responsible for the catastrophic scam of "Covid-19" merits the death penalty; as far I'm concerned their executions must be public, and televised: Nothing less is adequate.
No one knows what the long-term consequences for humanity of this orchestrated insanity will be. But they can't possibly be anything good.
The mask will likely increase the chances of respiratory illness and impeding breathing.